The Gulf Cooperation Council (GCC) states have changed dynamically over the past three decades and are on track for more transition. Individuals in this region have much to say about their own well-being and life experiences. Using subjective measures of health, such as evaluative well-being, and experiential measures, such as the incidence of health problems, pain, and depression, this paper studies the overall health of the GCC population and infers conclusions related to their potential effect on objective health measures.
Growth and progress in the GCC over the past three decades have brought improvements in infant mortality, life expectancy, and fertility rates.[1] Despite these improvements, the region is experiencing the type of health problems prevalent in high-income cultures, where substantial proportions of the population are sedentary. Increased obesity in children, adolescents, and adults, hypertension, and diabetes are recent health problems to which the GCC has had to adapt.[2]
Results for evaluative well-being outcomes were measured based on the Cantril Self-Anchoring Striving Scale, which asks individuals to rate their current and future lives on a ladder scale from 0 to 10.[3] On the ladder, 0 represents the worst possible life and 10 represents the best possible life. Individuals who rate their current lives a 7 or higher and their future lives an 8 or higher are classified as "thriving." Substantial proportions of nationals in each GCC country fall into the thriving category. Most GCC countries' thriving percentages are higher than the 43% median for high-income countries globally, although they range from 27% in Bahrain to 63% in the United Arab Emirates (UAE) and only Bahrain trails other high-income countries. Young people worldwide are generally more likely to be classified as thriving than older people from the same area. This trend is not evident in the GCC countries surveyed, as thriving is consistent across all age groups.
Results for experiential health outcomes were measured with items that ask about the pain respondents experienced the previous day, health problems, and depression. All of these measures are high relative to respondents' satisfaction with their own health, which ranges from 86% in Bahrain to 96% in the UAE. Individuals reporting negative health experiences (namely pain and depression) are less likely to be thriving. Overall findings support the use and importance of subjective individual measures of health in evaluating the health and well-being of the greater society, particularly those in a state of progress and change.
Context
Well-being is a vital aspect of the human experience. Without good health, individuals' quality of life and experiences are poor. The World Health Organization (WHO) defines health as a "state of complete physical, mental and social well-being and not merely the absence of disease or infirmity."[4] For several decades, governments have relied on objective measures, such as gross domestic product, life expectancy at birth, or diabetes prevalence, to gauge their citizens' wealth and health. While such metrics provide important information for assessing individuals' overall well-being at the national level, they cannot tell the whole story. Subjective measures of well-being are increasingly being incorporated into health studies.[5]
The Arabian Gulf countries represent a unique socio-economic cluster in the Middle East and North Africa (MENA) region. Stretching from the Red Sea to the Arabian Gulf, they encompass six countries (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates) that formed a cooperative framework in 1981 known as the Gulf Cooperation Council (GCC). The GCC countries have many common characteristics. They are all high-income, hydrocarbon-based economies. Their political systems, based on monarchies, are relatively similar. They also share a common language, religion, and social values. In addition, rapid economic growth and urbanization, brought about by oil and natural gas wealth, have accompanied important demographic and health changes over the past three decades.[6]
Since the 1980s, infant mortality-the number of children per 1,000 live births who die in the first 12 months of life-has declined significantly in all GCC countries. The infant mortality rate in the GCC country cluster was estimated at 37.7 per 1,000 live births in 1980-1985. Thirty years later, it is projected to fall to 11.8 per 1,000 live births.[7] Fertility rates have also declined greatly over the last several decades. Across the GCC, the total fertility rate, defined as the average number of children a woman has during her reproductive life, decreased from 5.8 children per woman in 1980-1985 to 3.5 in 2000-2005. The World Bank puts the current rate at 2.7; however, this fertility rate is still above the replacement level of about 2 children per woman across the MENA region. According to the latest Abu Dhabi Gallup Center report, Progress and Tradition in the Gulf Cooperation Council States, there are no clear indicators that that rate will decrease soon, as GCC men and women say four is the ideal number of children for a family to have. Additionally, as education attainment increases in the GCC, particularly for women, there is no notable decrease in family size. In some countries, such as Saudi Arabia, highly educated women report having three or more children at home.[8]
In addition to greater population growth, gains in life expectancy have been impressive. Between 1980 and 2005, life expectancy at birth increased from 65.3 years to 72.2 years for men, while it increased from 72.2 years to 76 years for women.[9]
The relatively high fertility rate in previous decades, combined with the decrease in mortality and the gains in life expectancy, have produced a large working-age cohort (people aged 15 to 64). The annual rate of population growth ranged from a high of 4.8% in the UAE to a low of 2.6% in Kuwait between 1980 and 2002. In 2010, the current GCC cluster population stands at 41.45 million, up from 29.63 million in 2000.[10] Though not the focus of this study, another important common characteristic of the GCC is the presence of significant proportions of Arab and non-Arab expatriate workers.
Along with these demographic changes, there have been important changes in nutrition and health across the GCC. Economics can influence diet patterns in powerful ways. As countries grow richer and more urban, people eat more fat and sugar. This phenomenon known as the "nutrition transition" is accompanied by a change in activity patterns, such as a more sedentary lifestyle. The nutrition transition has important health implications as it is also associated with an epidemiological transition.[11] Under the nutrition transition scenario, infectious and nutrient-deficiency diseases start to become less prevalent and noncommunicable diseases such as obesity, heart disease, diabetes, and some cancers become more common.[12]
According to the WHO, all GCC countries are in the advanced stage of the nutrition transition and, as such, they experience relatively "high levels of overweight and obesity, and moderate levels of undernutrition and micronutrient deficiencies in some population subgroups."[13] Rapid increases in obesity have been recorded among children, adolescents, and young adults.[14] But overweight and obesity rates among adults are also relatively high, particularly in Kuwait, Qatar, and Saudi Arabia. Hypertension and diabetes are also quite prevalent.[15]
Many factors influence people's health, and recent evidence suggests individuals' subjective well-being measures are important metrics that help foster a better understanding of perceived health and health outcomes. It should be noted that Sen argues patients' social experiences may limit their assessments of their health, especially when a medical condition is not sensory. As such, he cautions against an over-reliance on "internal" or subjective health assessments.[16] However, a large study of hypertensive patients with coronary artery disease showed that high systolic blood pressure, which is usually not considered a sensory condition, is associated with a higher likelihood of reporting fair or poor subjective well-being.[17]
Using a large international data set, Deaton found no correlation between life expectancy and health satisfaction. At the same time, he acknowledged that subjective health measures represent vital metrics of a key dimension of the human experience.[18] Further, a study in which patients with hypertension and coronary heart disease rated their well-being showed such a subjective measure of well-being was useful in identifying patients with increased risk for adverse health outcomes.[19]
In addition, "recent evidence from neurobiology show that one brain area, the amygdala, plays a pivotal role in processing social emotions […]" and that "other experimental evidence also shed more light on the pathways responsible for translating psychosocial experiences into physiological perturbations."[20] Another study showed that patients with depressive symptoms, even in the absence of depressive disorder, fared worse than patients with no chronic conditions in terms of their perceived health and pain, as well as physical, social, and role functioning.[21] In general, an individual's subjective positive reports of his or her health may or may not be objectively healthy; however, an individual's subjective negative reports of his or her health should cause concern.
Against this general backdrop, it is clearly important to study the multiple aspects of individuals' well-being in the GCC. There is a lack of health research in the GCC that can be used for cross-country comparisons. For example, a search of several databases, including Medline, PubMed Central, SSRN, Google Scholar, and Academic OneFile, produced no results for studies about health and subjective measures of quality of life in the GCC region.
Objective
This paper first seeks to provide a baseline measurement of subjective well-being in several GCC countries.[22] The dearth of quantitative research and the growing inclusion of quality of life measures in medical research studies underscore the importance of such subjective metrics. Governments in several high-income countries are also increasingly interested in incorporating quality of life measures, including well-being, to provide a more accurate picture of national prosperity.[23] High life evaluations are usually associated with higher incomes, education, and more positive views about one's health in many high-income countries. As all GCC countries are high-income countries, it becomes important to ascertain whether the picture of life in this region looks similar to that in wealthy countries, in key demographics. As such, the paper seeks to provide a socio-economic profile of subjective well-being across the Gulf region.
Descriptive statistics about health perceptions, including satisfaction with one's health and incidence of physical pain and depression, provide other valuable information to inform the healthcare policy debate in individual GCC countries. Potential gender, age, and income differences in health perceptions are particularly interesting. But the paper also considers other demographic variables such as education and employment status. Furthermore, the paper seeks to determine potential relationships between life evaluations and health perceptions. More specifically, the interest is in measuring the potential effect of self-reports of physical pain and depression on life evaluations across various age cohorts.
Main Outcome Measures
Gallup measures well-being internationally using the Cantril Self-Anchoring Striving Scale, which asks individuals to rate their current and future lives on a ladder scale from 0 to 10. On the ladder, 0 represents the worst possible life and 10 represents the best possible life. The scale has been used in various studies to assess well-being. The Cantril scale can be reported as individual items, mean scores, and as comparisons between life today and life in five years. For the purposes of this paper, the responses are classified into meaningful groups of thriving, struggling, and suffering.
Individuals who rate their current lives a 7 or higher and their future lives an 8 or higher are classified as "thriving." As such, thriving is a subjective well-being measure that combines people's assessments of their current and future lives. In other words, thriving incorporates individuals' expectations of a better future, which can be seen as a proxy for hope. Gallup's global well-being research conducted in more than 100 countries shows that at the country level, thriving correlates with income, education, and health.
Those who rate their current lives a 5 or a 6 and their future lives a 5 through a 7 are classified as "struggling." In general, they report more daily stress and worry about money more than thriving respondents. Struggling individuals report more than double the number of sick days. They are more likely to smoke and are less likely to eat healthily.
Individuals who fall in neither the thriving nor the struggling categories, those who rate their lives now and in the next five years poorly (4 and below on both), are classified as "suffering." Globally, suffering individuals are more likely to say they lack the basics of food and shelter, more likely to experience physical pain, and more likely to report feeling a lot of stress, worry, sadness, and anger. [24]
Furthermore, well-being is a multi-dimensional construct, encompassing not only objective clinical assessments, but also subjective reports of disability, function, and sensory symptoms. However, there may be important differences in the quality of life among individuals with similar health status. Testa and Simonson indicate that while the objective dimension provides the "patient's degree of health," the subjective components "translate that objective assessment into the actual quality of life experienced."[25]
Such life evaluation metrics are distinct from other subjective well-being measures, such as affect measures.[26] In this paper, two experiences measured are feeling "physical pain" and feeling "depression" a lot of the day before the survey. Experiential well-being seeks to capture individuals' emotions as close as possible to their actual occurrence, while evaluative well-being measures the way individuals remember their experiences after they are over. Two other health-related items used in this paper relate to satisfaction with one's personal health and perceptions of one's health (self-reports of having health problems that prevent respondents from doing things people their age can normally do).
This paper focuses on the thriving category of life evaluation among nationals in the five GCC countries surveyed (Bahrain, Kuwait, Qatar, Saudi Arabia, and the UAE).
Design and Sample
Data for this paper are drawn from the Gallup World Poll, an ongoing research initiative that surveys residents in more than 100 countries every year. The Gallup World Poll was launched in 2005. Five out of the six GCC countries are included in the World Poll. Research findings for Oman are not available as Gallup could not conduct the questionnaire in the country prior to spring 2011. Results are based on face-to-face and telephone interviews with at least 500 adult nationals (aged 15 and older) per country in Bahrain, Kuwait, Qatar, Saudi Arabia, and the UAE between February and December 2010.
Before survey fieldwork can begin, Gallup completes four key steps: question design, translation, training, and sampling.
Question design: Most items have a dichotomous ("yes or no") response set. This helps to minimize contamination of the data attributable to cultural differences in response styles and to facilitate cross-cultural comparisons.
Translation: The questionnaire is written in English and then translated into Arabic. Two translators who are proficient in the original and target languages complete independent translations of the survey into the target language with the aim of conceptual equivalence of words or phrases. A third translator reviews the translated versions against the original version to agree on a common translation. That translation is then back-translated into English, and adjustments or discrepancies are resolved. Final confirmations of valid translations are submitted to Gallup for each local translation needed.
Training: Traditionally, Gallup selects local research partners who have experience conducting nationwide public opinion studies. In locations where public opinion polling is a relatively recent research activity, Gallup conducts extensive training to ensure that local partners are adequately prepared for the polling work. Gallup conducts in-depth training sessions with local field staff prior to the start of data collection. Topics covered in training include household selection, respondent selection, correct questionnaire administration, and other field quality procedures. The training sessions provide examples of best practices and standards required to ensure high quality when data are collected.
Sampling: Samples are probability-based, and in most countries, they are nationally representative of the resident population, aged 15 and older. Because of the relatively large proportion of foreign workers in GCC countries, Gallup collects quotas where the proportions of nationals are less than 50%. As such, the number of national adult respondents in each GCC country surveyed is less than 1,000. Both urban and rural areas are included in the fieldwork. Only areas where the safety of the interviewing staff is threatened, scarcely populated islands, and areas that interviewers can reach only by foot, animal, or small boat are excluded.
With the exception of Qatar, face-to-face surveys are used for Gallup World Poll research in GCC countries. The first stage of sampling is the identification of PSUs (Primary Sampling Units) consisting of clusters of households. PSUs are stratified by population size and/or geography, and clustering is achieved through one or more stages of sampling. Where population information is available, sample selection is based on probabilities proportional to population size; otherwise, simple random sampling is used.
Gallup uses random route procedures to select sampled households. Unless an outright refusal occurs, wherever possible, interviewers must make at least three attempts to survey the sampled household. Attempts occur on different days, and if local custom permits, at least one attempt occurs during a weekend. After three attempts, if interviewers cannot obtain an interview at the initial sampled household, they select the household to the immediate right of the initial household. If the first attempt at this household is unsuccessful, then interviewers select the house immediately to the left of the initial household.
Respondents are randomly chosen within the selected households. Interviewers list all eligible household members and their ages or birthdays and select the respondent by means of the Kish grid. The person who answers the door is not informed of the selection criteria until after the respondent has been identified.
In Qatar, computer-assisted telephone interviewing (CATI) interviews were conducted using landline and cellular telephones. For the first half of the sample, landline telephone numbers using random digit dialing (RDD) were used, which resulted in reaching a higher proportion of Arab expatriate households than Qatari national households. For the second half of the sample, cellular telephone numbers via RDD were called to increase the odds of reaching Qatari national households. At least three attempts were made to reach a person in each household, spread over different days and times of day.
The standardization procedures used in the translation and training phases are vital to ensuring that the questions asked of one population are comparable to another population. After data collection is complete, base sampling weights are constructed using population statistics to weight the data by gender, age and, where reliable data are available, by education or socio-economic status.
Data Weighting: Gallup uses data weighting to ensure a nationally representative sample for each country. This data weighting is intended to be used for calculations within a country. First, Gallup constructs base sampling weights to account for household size. Weighting by household size (number of residents aged 15 and older) allows Gallup to adjust for the probability of selection, as residents in large households will have a disproportionately lower probability of being selected for the sample. Second, Gallup constructs post-stratification weights. Gallup uses population statistics to weight the data by gender, age, and, where reliable data are available, education or socio-economic status. Finally, Gallup calculates approximate study design effect and margin of error. The design effect calculation reflects the influence of data weighting and does not incorporate the intra-class correlation coefficients. Specifically for the Gulf countries, where there is a substantial expatriate population, Gallup calculates weighting separately for the national population based on national targets and the expatriate population based on available targets for these groups. Only results for nationals are reported in this paper, so the weighting applied to this group allows for analysis void of the expatriate populations.
Gallup calculates the maximum margin of error around reported proportions for each country-level data set, assuming a 95% confidence level. The margin of error also includes the approximate design effect for the total country sample. The calculations of the response rates for each country follow AAPOR's standard definition (RR3). The response rate from the five GCC countries ranged from a high of 87% in Bahrain to a low of 50% in Kuwait.
Gallup independently funds the World Poll, including the questionnaire design, data collection, weighting, and analysis.
Results
Across the five GCC countries surveyed in 2010, there was a large range in life evaluations.[27] Life evaluations are highest in the UAE, where about two-thirds of nationals are classified as thriving. Life evaluations are lowest in Bahrain, where slightly more than one-quarter of nationals fall into the thriving category. Bahrainis' evaluative well-being-in terms of thriving and struggling individuals-is nearly the mirror opposite of Emiratis' well-being. In Qatar, 56% of nationals are classified as thriving, while 42% fall into the struggling category. Thriving and struggling are split in Saudi Arabia, 43% and 52%, respectively. A slight majority of nationals in Kuwait are classified as struggling, while 44% are thriving.
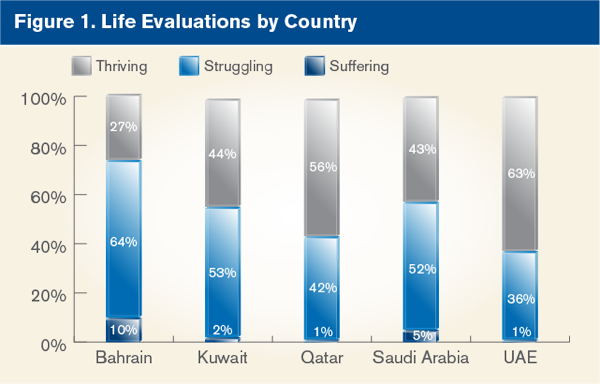
Suffering individuals are relatively rare, about 1% or 2% of the total population of nationals in Kuwait, Qatar, and the UAE. However, in Saudi Arabia, 5% of nationals are classified as suffering, and in Bahrain, the proportion of the population suffering is 10%.
Demographic Differences
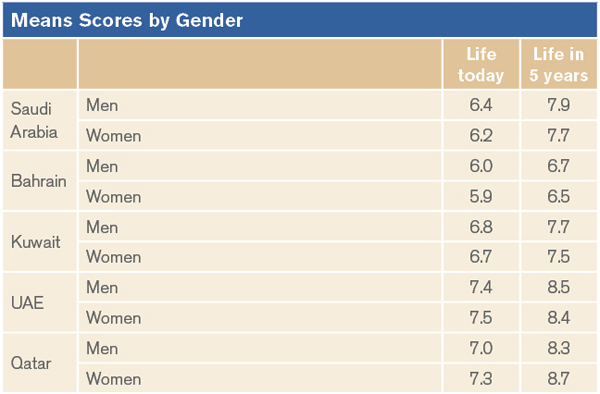
There are several demographic distinctions that are unique to GCC countries when examining thriving by age, gender, and education. In brief, more women are thriving than men. Young people are thriving at a rate no high or lower than other age categories. Thriving is consistent across all educational categories. Details of life today and life in five years are provided in Appendix A.
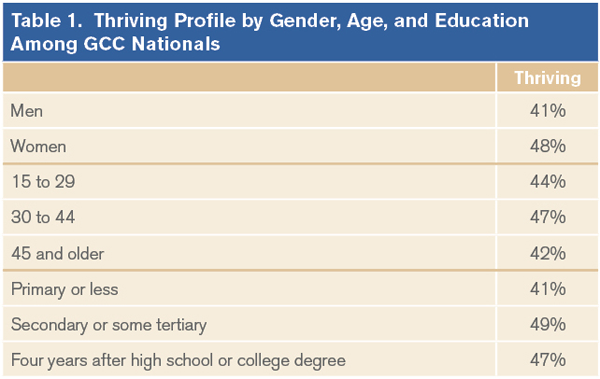
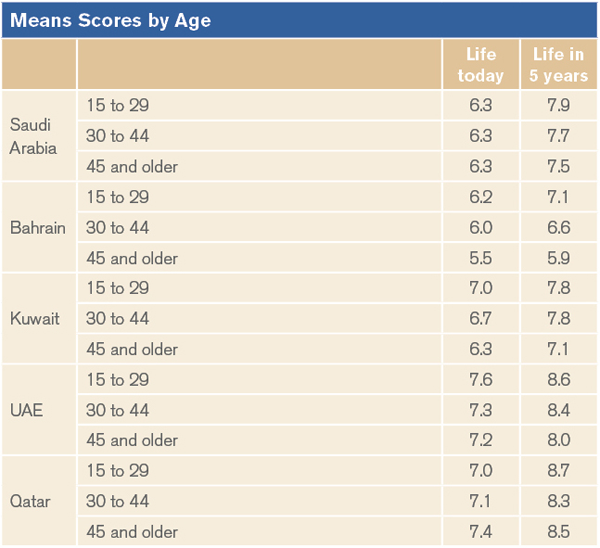
The demographic profile of thriving GCC nationals revealed several surprises at the aggregated level. First, the proportion of thriving individuals remains similar across age cohorts. Forty-four percent of those aged 15 to 29, 47% of those aged 30 to 44, and 42% of GCC nationals who are 45 and older are classified as thriving. The percentage-point differences are not statistically significant. Gallup's research conducted in more than 130 countries has shown that younger individuals around the world are far more likely to be thriving than older individuals, although in high-income countries such as the United States and the United Kingdom, life evaluations follow a U-shape pattern. They are high among the youngest age cohort, then decrease in middle age, and increase again after middle age.[28]
The lack of higher thriving levels among the younger age cohorts is particularly striking in Saudi Arabia. Forty-two percent of younger Saudis (those aged 15 to 29 as well as those aged 30 to 44) are classified as thriving, while 45% in the oldest age cohort (those 45 and older) fall into the same category. This lack of higher thriving among young people is also apparent in Qatar and the UAE. In Kuwait, however, there appears to be a slight linear relationship between life evaluations and age. A little more than one-half of Kuwaitis (52%) aged 15 to 29, 43% of those between the ages of 30 and 44, and 31% of Kuwaitis who are at least 45 years old are classified as thriving. In Bahrain, while there is no difference in thriving between the two youngest age cohorts (31% and 29%, respectively), people in both age groups are still more likely to be thriving than Bahrainis aged 45 and older (20%). Full age data on life today and life in five years can be found in Appendix A.
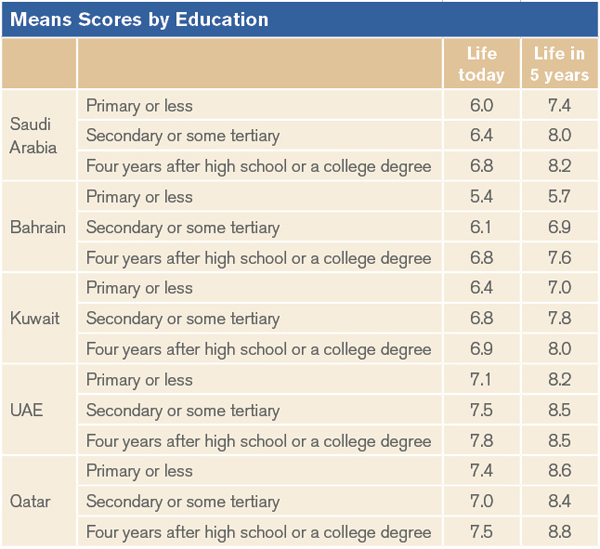
Education is another variable that does not appear to be strongly related to thriving when analyzing the aggregated data. GCC nationals with a secondary or some tertiary education (49%) or four years of education beyond high school or a college degree (47%) are no more likely to be thriving than those with a primary education or less (41%). The percentage-point difference is not statistically significant. However, in Bahrain and Kuwait thriving increases with higher levels of education. Fifty percent of Bahrainis with four years of education after high school or a college degree are thriving, compared with 35% of those with a secondary or some tertiary education and 27% of those who have a primary education or less. Fifty-one percent of Kuwaitis with a secondary or some tertiary education are thriving (the sample size of those who reached a higher level is too small to report results), compared with 29% of those with a primary level or less.
Gender is one demographic variable that shows important differences. Across the GCC, women are slightly more likely than men to be classified as thriving, 48% vs. 41%, respectively. When analyzing the country-level data, some interesting differences emerge. Women in Saudi Arabia (48%) and especially Qatar (64%) are far more likely than men (38% and 44%, respectively) to be thriving. There are, however, no gender thriving differences in the other three countries surveyed.
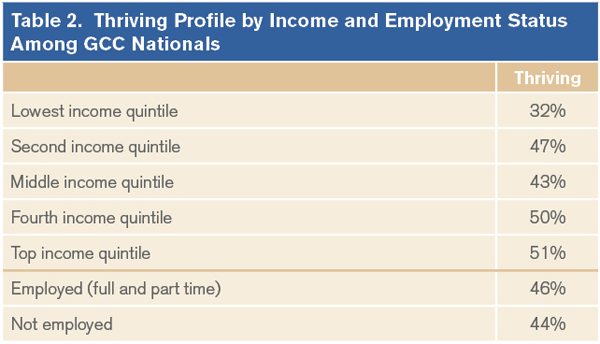
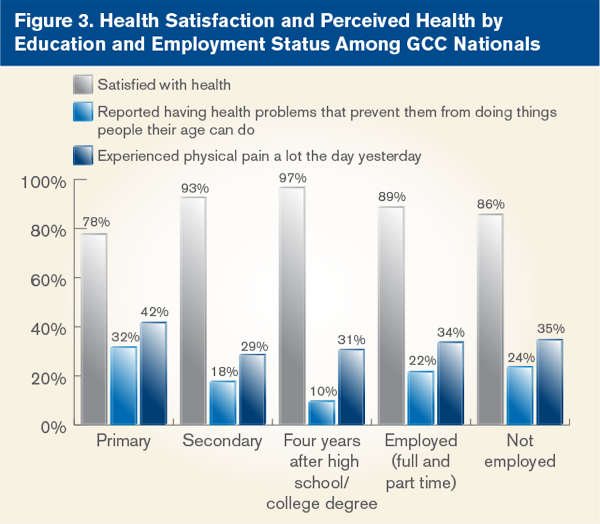
Another key finding is the lack of difference in thriving based on employment status. Usually, those who work for an employer are far more likely to be classified as thriving than those who are not employed.[29] Across GCC countries surveyed, 46% of employed (full and part time) nationals, compared with 44% of those who are not employed, are classified as thriving. This is particularly interesting as thriving is highly correlated to income around the world.[30] Within the GCC cluster, however, there are two exceptions. Employed Bahrainis (42%) and Kuwaitis (51%) are far more likely to be thriving than nationals who are not working, 28% and 41%, respectively.
In fact, the relationship between income and thriving in the GCC cluster is complex. While it is true that nationals in the top income quintile are far more likely to be thriving than those in the bottom quintile, 51% vs. 32%, a linear progression showing higher well-being as income increases is absent from the cluster of countries surveyed. Such a finding is borne out by results that show while average life satisfaction increases with GDP per capita, once a certain level is reached (more than $12,000), such life satisfaction shows only marginal increases, if any.[31]
Perceived Well-Being
In terms of well-being, or more specifically, perceived health, the results paint a mixed picture. On one hand, strong majorities of nationals in countries surveyed express satisfaction with their personal health. On the other, significant proportions report having experienced physical pain a lot of the day before the survey and many also say they have health problems that prevent them from doing things people their age can normally do. Satisfaction with one's health ranges from a high of 96% in the UAE to a low of 86% in Bahrain.
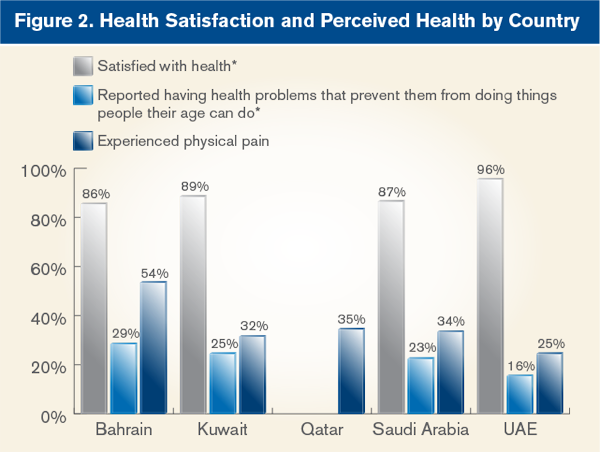
Reports of physical pain range from 25% in the UAE to 54% in Bahrain. In addition, reports of having health problems that prevent GCC nationals from doings things people their age can normally do range from 16% in the UAE to 29% in Bahrain. In general, the results show there are no gender, employment status, or even income differences in terms of health satisfaction and reports of health problems or physical pain. Bahrain presents a different case. Gender, employment status, and income differences in Bahrainis' health perceptions are significant and meaningful. Bahraini women (61%) are more likely than Bahraini men (48%) to report experiencing physical pain a lot of the day before the survey. Twenty percent of Bahrainis who work for an employer versus 36% of those who are not in the workforce say they have health problems that prevent them from doing things people their age can do. Bahrainis' employment status also seems to matter in their satisfaction with their health: 94% of Bahrainis who work for an employer express satisfaction with their personal health versus 81% of those not employed. With respect to income, Bahrainis in the top two income quintiles report much higher satisfaction with their personal health and are least likely to say they have health problems.
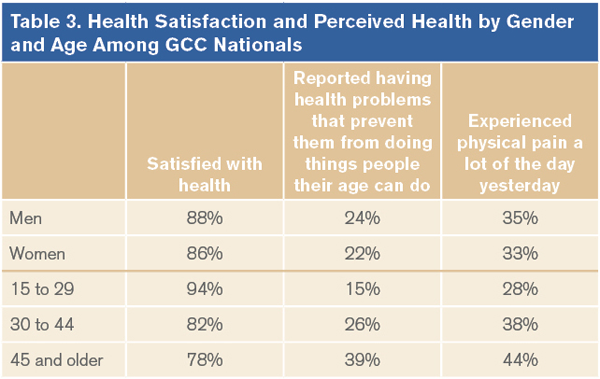
Education and age are important discriminating factors with respect to health satisfaction and perceived health across all GCC countries Gallup surveyed. Overall, those with a primary level of education or less are far less likely to say they are satisfied with their health than those with a secondary education or higher. In Saudi Arabia, 93% of those with a secondary or some tertiary education and 78% of those with primary education or less say they are satisfied with their personal health. Conversely, GCC nationals with at least a secondary education are far less likely than those with less education to report having health problems or experiencing physical pain a lot of the previous day. For instance, 19% of Saudis with a secondary or some tertiary education, compared with 31% of those with a primary or less education, say they have health problems that prevent them from doing things people their age can do. Similarly, Saudis with more education are almost twice as less likely as those with a primary level to report feeling physical pain a lot the day before.
The relationship between people's age and their satisfaction with their health is not unique to the GCC. Globally, people's satisfaction with their health decreases as they grow older, with the decline in health satisfaction more pronounced in low- and middle-income countries than in richer economies, perhaps because of the role income plays in softening the effects of aging on individuals' perceptions of their own health.[32] But differences in health satisfaction by age vary in GCC countries surveyed.
When examining the sample by three age categories, young (15 to 29), middle-aged (30 to 44), and older (45 and older), Gallup looks for a gradual linear decrease in health satisfaction with advancing age. In Saudi Arabia, while the youngest nationals are far more likely than older nationals to express satisfaction with their health, the percentage-point difference between those aged 30 to 44 and those 45 and older is not significant. In Bahrain and Kuwait, younger nationals are more likely than older ones to express satisfaction with their health, but there are no significant differences between the youngest and middle-age cohorts. Bahrain also records the largest drop in health satisfaction between the youngest and oldest age cohorts (19 percentage points) of all the GCC countries surveyed. In the UAE, the sample size for those aged 45 and older is too small to report results. Younger Emiratis are far more likely to express satisfaction with their health than those who are 45 and older.
Although the youngest nationals across the GCC are far less likely than the oldest ones to say they have health problems that prevent them from doing things people their age can do, such reports usually do not show a progressive, linear increase with age. Saudi Arabia is the notable exception: 15% among those aged 15 to 29, 27% among those aged 30 to 44, and 39% among those 45 and older say they have health problems that prevent them from doing things people their age can do. In Bahrain, Kuwait, and the UAE, middle-aged nationals are as likely as those aged 15 to 29 to report having such health problems.
Reports of feeling a lot of physical pain also show an inconsistent pattern with age across the countries surveyed. In Qatar, there is no significant difference on this issue between the youngest and the middle-age cohort. But it is important to note that a sizable proportion of Qataris aged 15 to 29 (36%) reported feeling physical pain a lot of the previous day. The sample size of Qataris aged 45 and older is too small to report results. In both Bahrain and Kuwait, reports of physical pain increase as nationals grow older. Bahrain is also where reports of physical pain are, in general, the highest among GCC countries surveyed, regardless of the age cohort. But in the UAE, there is no difference in physical pain reports between Emiratis aged 30 to 44 and those 45 and older.
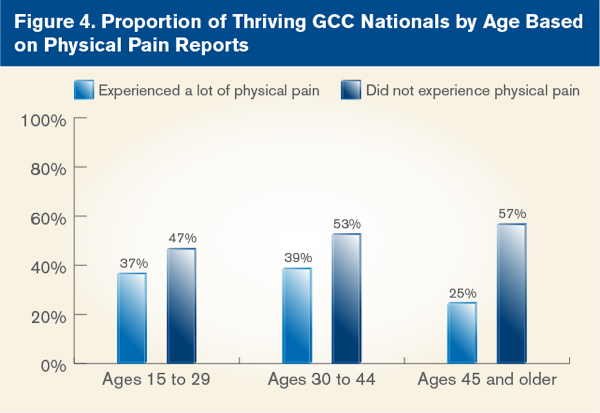
Factors influencing thriving have shown, at least at the country level, the importance of health perceptions, especially in terms of physical pain (or lack thereof) among men and women in three of the five countries surveyed.[33] For example, in Kuwait and the UAE, reporting a lack of physical pain is a top predictor of positive life evaluation for both men and women. Reporting an absence of physical pain yesterday is also a top thriving predictor among men in Bahrain and Saudi Arabia. As physical pain can increase with age, one can analyze how it relates to thriving among the different age cohorts. Physical pain appears to affect thriving more among those aged 45 and older.
Furthermore, a specific health condition, depression-although it does not represent a clinical diagnosis as it is reported by the respondents-affects life evaluations. Self-reports of depression in the GCC are higher than depression reported in other high-income countries. The high-income country median for not experiencing depression yesterday is 92% for men and 89% women.
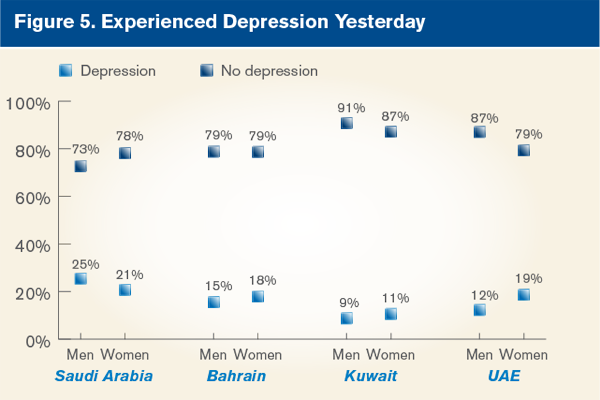
Thriving is reported far less among those individuals who report experiencing depression the previous day. Across all GCC nationals, half of the population (50%) that did not experience depression reported thriving (50%) while 24% of those who said they experienced depression could be classified as thriving. Depression differences in thriving are the least evident among men and women 45 and older.
The difference between experiencing depression and not experiencing depression has a greater effect on men's thriving than women's thriving. Women who reported experiencing depression are consistently less likely to be thriving, regardless of age. A 21-percentage-point difference separates young and middle-aged women who are experiencing depression from women in the same age groups who are not experiencing depression.
The effect is larger for men in the two younger age categories. For men 15 to 29 there is a 28-percentage-point drop in thriving between men who did not experience depression and men who did experience depression. Men in the 30 to 44 age group similarly were 31 percentage points lower in thriving if they experienced depression the day before. When examining depression's relationship to overall well-being, the relationship with thriving for men in these two age categories is evidence of the importance of mental health factors in addition to more traditional physical health indicators.
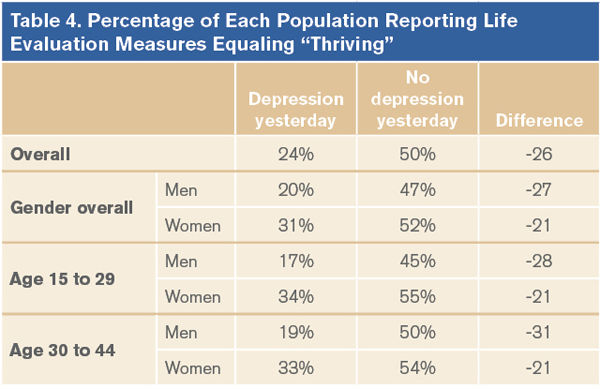
Results show that self-reports of depression are important in life evaluation measures across young and middle-aged cohorts.
Discussion
Measuring subjective well-being is uniquely important in the GCC given the dynamic population change these countries have experienced over the past three decades. Tracking this change over time is particularly important to monitor high- and low-income groups and life satisfaction.[34] The coming decades promise more transformation and provide a continued reason to follow subjective health metrics and a more global metric of well-being. The addition of subjective health measures to any analyses of well-being and health in the GCC is pivotal as individual health within these countries is transitioning with their respective economy and infrastructure.
From the research presented, Gallup knows that subjective measures of health, such as life evaluations, physical pain, depression, and satisfaction with personal health, are a gateway to assessing a population's overall well-being. Generally high satisfaction with health across GCC countries is not manifesting itself in positive health reporting. When Gallup examines rates of physical pain and depression, it finds that these are high in the GCC countries relative to other high-income countries around the world. Populations that tend to be protected from such health issues, including young people, are not seeing relief from health issues across the GCC. Young people in the GCC are experiencing pain and depression at rates fairly similar to those in the middle-aged group.
As a result of the important demographic and epidemiological changes and challenges for well-being in the GCC, healthcare services must adapt to address the effects of the nutrition transition. Through that adaptation, the effective use of subjective measures of well-being can play a vital role. Furthermore, the inclusion of subjective well-being metrics in well-being studies offers the potential to investigate not only their relationships with chronic diseases, but also presents the opportunity to study populations who are relatively free of diseases.
Failure to address the significant proportions of the GCC population who are experiencing physical pain, depression, and health problems that prevent them from doing things people their age can do will have direct costs to the overall health of the GCC people and their economies. In addition to the relationship these health issues have with decreased thriving, they could also likely have substantial economic costs. There are already estimates that healthcare spending for the GCC will reach $60 billion U.S. by 2025. This would be an increase of $48 billion from its current estimate of $12 billion.
Against this backdrop, subjective well-being measures could serve as a vital metric with which to gauge progress toward healthier societies in the region.
References
Abu Dhabi Gallup Center. 2011. Progress and Tradition in the Gulf Cooperation Council States: Exploring the unique assets and challenges in a rapidly changing region.
Cantril, Hadley. 1965. The pattern of human concerns. New Brunswick, NJ: Rutgers University Press.
Clifton, J., and Marlar, J. 2011. Good Jobs: The New Global Standard. Gallup. Washington, D.C.
Deaton, Angus. 2008. Income, health, and well-being around the world: Evidence from the Gallup World Poll. Journal of Economic Perspectives 22 (2): 53-72.
Drewnowski, A., and Popkin, B. 1997. The Nutrition Transition: New Trends in the Global Diet. Nutrition Reviews 55 (2):31-43.
Economic and Social Commission for Western Asia (ESCWA). 2007. Population ageing in Arab countries. United Nations, New York, NY.
Gallup. 2011. Worldwide Research Methodology and Codebook. April 2011. Washington, D.C.
Gong, Y., Hanberg, E.M., Gerhard, T., Cooper-DeHoff, R.M., Ried, L.D., Johnson, J.A., and Pepine, C.J. 2009. Systolic blood pressure and subjective well-being in patients with coronary artery disease. Clinical Cardiology 32 (11): 627-32.
Kahneman, D., Krueger, A., Schkade, D., Schwarz, N., and Stone, A. 2006. Would you be happier if you were richer? A focusing illusion. Science 312:1908-10.
Kahneman, D., Diener, E., and Schwarz, N. (Eds.). 1999. Well-being: the foundations of hedonic psychology. New York: Russell Sage Foundation.
Khatib, O. 2004. Noncommunicable diseases: risk factors and regional strategies for prevention and care. Invited paper. La Revue de Santé de la Méditerranée orientale. 10 (6):778-88.
Ng, S.W., Zaghloul, S., Ali, H.I., Harrison, G. and Popkin, B.M. 2010. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obesity Reviews 12:1-13.
Popkin, B. 2006. Global nutrition dynamics: the world is shifting rapidly toward a diet linked with noncommunicable diseases. The American Journal of Clinical Nutrition 84:289-98.
Report by the Commission on the Measurement of Economic Performance and Social Progress. 2009.
Ried, L.D., Tueth, M.J., Handberg, E., and Nyanteh, H. 2006. Validating a self-report measure of global subjective well-being to predict adverse clinical outcomes. Quality of Life Research 15:675-86.
Roy, J. 2004. Socioeconomic status and health: a neurobiological perspective. Medical Hypotheses 62:222-27.
Sen, A. 2002. Health: perception versus observation. British Medical Journal 324: 860-1.
Testa, M.A., and Simonson, D.C. 1996. Assessments of quality-of-life outcomes. The New England Journal of Medicine 334 (13): 835-840.
Wells, K., Stewart, A., Hays, R., Burnam, A., Rogers, W., Daniels, M., Berry, S., Greenfield, S., and Ware, J. 1989. The Functioning and Well-being of Depressed Patients. JAMA 262:914-19.
Wilson, I., and Cleary, P. 1995. Linking Clinical Variables with Health-Related Quality of Life JAMA 273:59-65.
World Health Organization. 2010. Regional strategy on nutrition 2010-2019. Technical paper. Regional Committee for the Eastern Mediterranean. EM/RC57/4.
Question Wording
Please imagine a ladder with steps numbered from 0 at the bottom to 10 at the top. Suppose we say that the top of the ladder represents the best possible life for you, and the bottom of the ladder represents the worst possible life for you.
On which step of the ladder would you say you personally feel you stand at this time, assuming that the higher the step the better you feel about your life, and the lower the step the worse you feel about it? Which step comes closest to the way you feel?
Just your best guess, on which step do you think you will stand in the future, say about five years from now?
10 Best possible life
09
08
07
06
05
04
03
02
01 Worst possible life
Don't know
Refused
Are you satisfied or dissatisfied with your personal health?
Satisfied
Dissatisfied
Don't know
Refused
Do you have any health problems that prevent you from doing any of the things people your age normally can do?
Yes
No
Don't know
Refused
Did you experience the following feelings during A LOT OF THE DAY yesterday? How about…physical pain?
Yes
No
Don't know
Refused
Did you experience the following feelings during A LOT OF THE DAY yesterday? How about…depression?
Yes
No
Don't know
Refused
Appendix A
Abu Dhabi Gallup Center
The Abu Dhabi Gallup Center is a Gallup research hub based in the capital of the United Arab Emirates. It is the product of a partnership between Gallup, the world's leading public opinion research firm, and the Crown Prince Court of Abu Dhabi.
Building on Gallup's seminal work in the field of Muslim studies, the Abu Dhabi Gallup Center (ADGC) offers unmatched research on the attitudes and aspirations of Muslims around the world. In addition to its worldwide scope, the ADGC focuses on the specific priorities of its regional base and presents innovative analysis and insights on the most important societal challenges facing the United Arab Emirates and the Gulf Cooperation Council (GCC).
[1] Economic and Social Commission for Western Asia. "Population ageing in Arab countries." (New York, NY: United Nations, 2007).
[2] S.W. Ng, S. Zaghloul, H.I. Ali, G. Harrison, and B.M. Popkin, "The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States," Obesity Reviews (2010): 12:1-13.
[3] Hadley Cantril, "The pattern of human concerns." (New Brunswick, NJ: Rutgers University Press, 1965).
[4] World Health Organization. Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, June 19-22, 1946, and entered into force on April 7, 1948.
[5] Ira Wilson and Paul Cleary, "Linking clinical variables with health-related quality of life." JAMA (1995), 273:59-65.
[6] Economic and Social Commission for Western Asia, "Population ageing in Arab countries."
[7] Ibid.
[8] Abu Dhabi Gallup Center. "Progress and Tradition in the Gulf Cooperation Council States: Exploring the unique assets and challenges in a rapidly changing region." Gallup (2011).
[9] Economic and Social Commission for Western Asia. "Demographic profile of the Arab countries." (New York, NY: United Nations, 2009).
[10] Jane Kinninmont, "The GCC in 2020: Outlook for the Gulf and the global economy." Economist Intelligence Unit, 2009.
[11] Barry Popkin, "Global nutrition dynamics: the world is shifting rapidly toward a diet linked with noncommunicable diseases." The American Journal of Clinical Nutrition (2006): 84:289-98.
[12] Adam Drewnowski and Barry Popkin, "The nutrition transition: new trends in the global diet." Nutrition Reviews (1997): 55 (2):31-43.
[13] World Health Organization. Regional strategy on nutrition 2010-2019. Technical paper. Regional Committee for the Eastern Mediterranean. EM/RC57/4. 2010.
[14] O. Khatib, "Noncommunicable diseases: risk factors and regional strategies for prevention and care." Invited paper. Eastern Mediterranean Health Journal (2004): 10 (6):778-88.
[15] S.W. Ng, et al. Obesity Reviews (2010): 12:1-13.
[16] Amartya Sen, "Health: perception versus observation." British Medical Journal (2002): 324: 860-1.
[17] Y. Gong, E.M. Hanberg, T. Gerhard, R.M. Cooper-DeHoff, L.D. Ried, J.A. Johnson, and C.J. Pepine, "Systolic blood pressure and subjective well-being in patients with coronary artery disease." Clinical Cardiology (2009): 32 (11): 627-32.
[18] Angus Deaton, "Income, health, and well-being around the world: Evidence from the Gallup World Poll." Journal of Economic Perspectives (2008): 22 (2): 53-72.
[19] L. Douglas Ried, Michael J. Tueth, Eileen Handberg, and Harry Nyanteh, "Validating a self-report measure of global subjective well-being to predict adverse clinical outcomes." Quality of Life Research (2006): 15:675-86.
[20] Jean-Pierre Roy, "Socioeconomic status and health: a neurobiological perspective." Medical Hypotheses (2004): 62:222-27.
[21] Kenneth Wells, Anita Stewart, Ron Hays, Audrey Burnam, William Rogers, Marcia Daniels, Sandra Berry, Sheldon Greenfield, and John Ware, "The functioning and well-being of depressed patients." JAMA (1989): 262:914-19.
[22] Surveys were conducted in Bahrain, Kuwait, Qatar, Saudi Arabia, and the UAE only.
[23] Report by the Commission on the Measurement of Economic Performance and Social Progress. 2009.
[24] Gallup, "Worldwide research methodology and codebook." Washington, D.C.: April 2011.
[25] Marcia A. Testa and Donald C. Simonson, "Assessments of quality-of-life outcomes." The New England Journal of Medicine (1996): 334 (13): 835-840.
[26] Daniel Kahneman, Ed Diener, and Norbert Schwarz (Eds.), "Well-being: the foundations of hedonic psychology." New York (1999): Russell Sage Foundation.
[27] Thriving respondents rate their present lives a "7" or higher and their future lives an "8" or higher on the Cantril Ladder scale, with steps numbered from "0" to "10." Struggling respondents rate their present lives a "5" or a "6" and their future lives on steps "5" through "7." Those classified as suffering rate their present and future lives on steps "0" through "4."
[28] Angus Deaton, "Income, health, and well-being around the world: Evidence from the Gallup World Poll." Journal (2008).
[29] Jon Clifton and Jenny Marlar, "Good jobs: The new global standard." Washington, D.C.: Gallup (2011).
[30] Angus Deaton, "Income, health, and well-being around the world: Evidence from the Gallup World Poll." Journal (2008).
[31] Daniel Kahneman, Alan Krueger, David Schkade, Norbert Schwarz, and Arthur Stone, "Would you be happier if you were richer? A focusing illusion." Science (2006): 312:1908-10.
[32] Angus Deaton, "Income, health, and well-being around the world: Evidence from the Gallup World Poll." Journal (2008).
[33] Abu Dhabi Gallup Center. "Progress and Tradition in the Gulf Cooperation Council States: Exploring the unique assets and challenges in a rapidly changing region." Gallup (2011).
[34] Angus Deaton, "Income, health, and well-being around the world: Evidence from the Gallup World Poll." Journal (2008).